Valve Surgery
Leading-Edge Diagnostics and Therapies
The WMCHealth Heart and Vascular Institute’s Valvular Heart Disease Program offers precise, cutting-edge care for patients with mild valvular pathology and critical disease requiring intervention. Our program treats the most cases in the Hudson Valley.
The presentation, diagnosis and treatment of valvular heart disease have steadily evolved for decades. Advances that relieved symptoms and improved prognosis in patients with aortic stenosis and high surgical risk have inspired new strategic approaches to valvular heart disease, and the WMCHealth Heart and Vascular Institute pioneered these advances in the Hudson Valley.
Pioneering Valvular Heart Disease Care in the Hudson Valley
Westchester Medical Center became the first local hospital to perform a transcatheter aortic valve replacement (TAVR). This commitment to innovation led to the Valvular Heart Disease Program, which brings together the expertise of imaging experts, highly skilled interventional cardiologists and accomplished cardiothoracic surgeons. This team-based approach ensures patients receive timely, dignified care optimizing the latest therapies.
The program is led by noninvasive cardiologist Daniel Spevack, MD; Director of Cardiothoracic Surgery Steven Lansman, MD, PhD; cardiac surgeon Joshua Goldberg, MD; and Hasan Ahmad, MD.
Westchester Medical Center, known for its state-of-the-art technology and equipment, recently opened its new Ambulatory Care Pavilion adjacent to the hospital’s main tower. The Ambulatory Care Pavilion provides a cutting-edge environment for patient testing and imaging, including transesophageal and transthoracic echocardiograms, and it is a showcase for the latest technologies from healthcare equipment leader Philips. Leading-edge imaging capabilities include technology that layers echocardiogram and catheterization images together, providing a powerful, precise diagnostic tool. The Ambulatory Care Pavilion also provides increased availability for patient appointments.
Mitral Valve Procedures
About the Mitral Valve
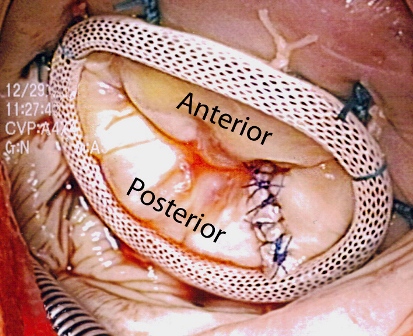
The mitral valve sits between the left atrium and left ventricle, and is comprised of two leaflets, anterior and posterior. When the mitral valve is open, it allows blood to pass from the atrium to the ventricle. When closed, it prevents blood from backing up into the atrium as the ventricle pumps blood out of the heart.
Normal mitral valve leaflets are thin, delicate structures that meet each other in a process known as coaptation. The edges of the anterior and posterior leaflets are attached to the papillary muscles in the left ventricle by thin fibrous strands called the chordae tendinae. Through this attachment, the opening and closing of the mitral valve is a dynamic process guided by the motion of the left ventricle. The mitral leaflets are anchored in the mitral annulus, which is part of the fibrous skeleton of the heart. The annulus provides the framework for the valve leaflets.
Mitral valve repair with Steven Lansman, M.D. Ph.D. Westchester Medical Center
Mitral Valve Pathology
When the mitral valve does not function properly, it can cause excessive leakage of blood back into the left atrium. In its most severe form, it can cause blood to back up into the lungs and cause deterioration of heart function. Together, these conditions are called congestive heart failure.
Leakage of the mitral valve, called mitral valve regurgitation, can be produced by a number of different pathologic conditions. Most commonly, excessive leaflet tissue prevents the leaflets from closing normally, leading to leakage of blood through the valve. Alternatively, the muscles or chordae that support the leaflets can rupture, which prevents normal valve closure. Finally, different adaptations to chronic heart failure can cause the annulus of the mitral valve to enlarge, thereby producing leakage.
Less commonly, other factors can prevent the mitral valve from opening enough, actually restricting the amount of blood that can flow through the valve. This condition, usually associated with rheumatic fever, is called mitral valve stenosis.
Mitral Valve Treatments
Mitral valve regurgitation can be successfully treated with surgery, and, if performed early enough, can limit progression of congestive heart failure. If you have mitral valve regurgitation, your cardiologist should discuss the various treatments available to you, including medical therapy as well as surgery. There are two surgical options for treatment for mitral valve regurgitation -- mitral valve repair and mitral valve replacement.
Mitral Valve Repair
While initially, most valves had to be replaced, the mitral valve can now be successfully repaired in over 90% of patients with mitral valve regurgitation. Mitral valve repair has significant advantages over replacement, as it is associated with better long term outcomes and less need for future surgery. Repair techniques are varied, but generally involve reconstructing the patient's own valvular tissue to produce better coaptation of the valve leaflets. Additionally, a ring or band is placed in the mitral annulus, which provides structural support for the repaired valve.
Mitral valve repair can now be performed using small incisions in the chest, avoiding the need for a sternotomy. Using some specialized instruments, the mitral valve can be repaired using the exact same techniques that are used in the standard approach. Using these less invasive techniques, patients may experience less pain and may return to their normal activities sooner.
Mitral Valve Replacement
Early in the history of mitral valve surgery, replacement of the valve was the most commonly performed treatment. It is still performed today, and the valve replacements fall into two general categories, mechanical valves and bioprosthetic ("tissue") valves. While mechanical valves have a long lifespan, patients will need to be treated with blood-thinners (i.e. coumadin) for the rest of their lives. Bioprosthetic valves can last 10-15 years, but patients do not need any treatment with blood-thinners. Mitral valve replacement surgery is generally indicated in those patients with advanced rheumatic valvular disease or significantly calcified valves, for whom mitral valve repair surgery is not possible.
For additional information please call 866.WMC.HEART or 866.962.4327
Our Address
Westchester Medical Center
Ambulatory Care Pavilion
100 Woods Road
Valhalla, NY 10595
Directions
By Car
By Train
Westchester Medical Center is served by Metro North's Harlem line via two stations:
- White Plains - Bus transfer options available
- Hawthorne - Taxi service available
For train fare and schedule information, call 1-800-METRO-INFO or go to mta.info/mnr .
By Bus
There are three bus lines (Westchester Bee Line) you can take to our campus. Please call 914.813.7777 for bus routes and fares.
Campus Map
The Westchester Medical Center campus includes the Maria Fareri Children's Hospital and the Behavioral Health Center.